Decoding the Diagnosis: Understanding Breast Cancer Stages & Types in 2026
The Call You Never Want to Get
"It's malignant." The moment those words hang in the air, the world seems to stop spinning. You enter a new universe—one filled with medical jargon, endless appointments, and fear.
But here is the truth: Information is the antidote to fear.
This guide is your translator. Doctors speak in codes (TNM, ER, PR, HER2, Grade). In 2026, personalized medicine means that "Breast Cancer" isn't just one disease; it is hundreds of unique subtypes, each with a specific roadmap. We are here to decode the map so you can reclaim control.
Part 1: The Biology of YOUR Cancer
Before looking at staging, you must understand the personality of your tumor. Two women with Stage 2 cancer can have completely different treatments based on the biology.
The Receptors (The "Fuel" System)
Think of the cancer cell as a customized house. On the outside of this house, there are "doorbells" or specific locks. These are receptors. If we know what keys unlock the growth, we can block them.
- ER+ (Estrogen Receptor Positive):
- The Fuel: Estrogen. The cancer cells have receptors that grab estrogen from your blood and use it to grow.
- The Treatment: Anti-hormonal therapy (Tamoxifen, Aromatase Inhibitors) acts like gum in the lock, preventing estrogen from entering.
- Commonality: ~80% of all breast cancers.
- PR+ (Progesterone Receptor Positive):
- The Fuel: Progesterone.
- Similarities: Often found together with ER+.
- HER2+ (Human Epidermal Growth Factor Receptor 2):
- The Fuel: The HER2 protein. Normal cells have a few copies; these cancer cells have too many (amplification).
- Personality: Fast-growing and aggressive.
- The Good News: Pre-2005, this was the worst diagnosis. Now, thanks to targeted drugs like Herceptin (Trastuzumab), it is one of the most treatable forms. It is the "poster child" for targeted therapy.
The "Triple Negative" (TNBC)
- The Status: ER-, PR-, HER2-. This means the cancer tests negative for all three common receptors.
- The Challenge: Because it lacks the "doorbells," hormonal pills and Herceptin don't work.
- The Plan: Chemotherapy is the primary weapon.
- The Silver Lining: TNBC is often "chemosensitive," meaning it melts away faster with chemo than other types. New immunotherapy drugs (Keytruda) approved in the last few years have radically improved survival rates for Stage 2 & 3 TNBC.
Part 2: The Stages (0 to 4) – How Far Has It Gone?
Staging is usually determined by the TNM System, updated recently in the AJCC 8th Edition to include biological factors (not just size).
- T (Tumor): How big is the mass?
- N (Node): has it traveled to the lymph nodes?
- M (Metastasis): has it traveled to distant organs?
Sate 0: DCIS (Ductal Carcinoma In Situ)
- Theory: "Stage 0." Cancer cells have formed inside the milk duct but have not broken through the wall into the surrounding tissue. They cannot spread yet.
- Treatment: Surgery (Lumpectomy) usually followed by Radiation.
- Survival: Nearly 100%.
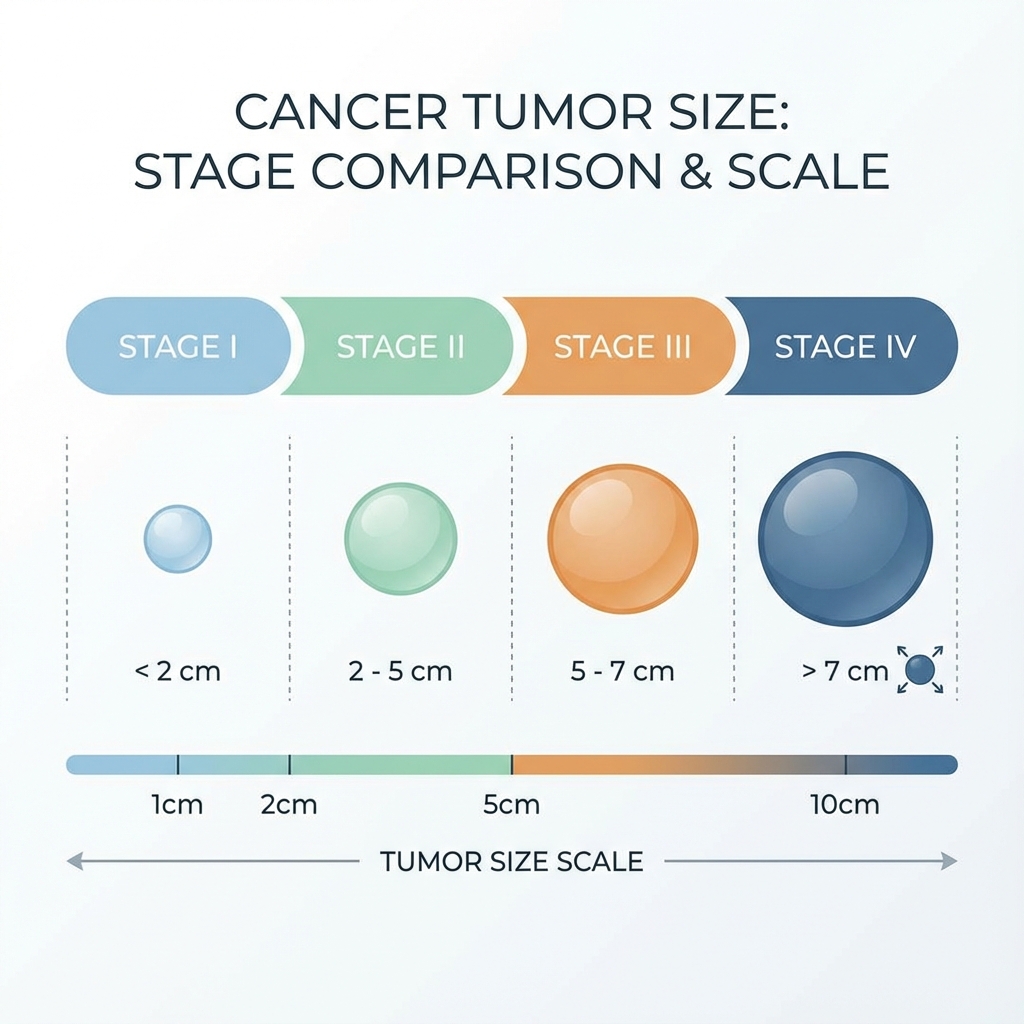
Stage 1: Small & Contained
- 1A: Tumor is small (< 2cm) and nodes are clear.
- 1B: Tiny clusters of cells found in lymph nodes (micrometastasis).
- Prognosis: Excellent. Often treated with surgery and radiation alone (no chemo), depending on the Oncotype score.
Stage 2: The Grey Zone
- Tumor is larger (2-5cm) OR has spread to 1-3 lymph nodes.
- The Debate: Chemotherapy is often debated here.
- Neoadjuvant: Many doctors now give Chemo before surgery for Stage 2 to shrink the tumor and test if the drugs work.
Stage 3: Locally Advanced
- Tumor is large (> 5cm) OR has spread to many lymph nodes (4+) or chest wall/skin.
- Goal: Curative. The treatment is aggressive and "throws the kitchen sink" at it.
Stage 4: Metastatic (MBC)
- The cancer has left the breast area and planted seeds in the bones, liver, lungs, or brain.
- Paradigm Shift: In 2026, Stage 4 is treated as a chronic illness, much like diabetes. Women are living 5, 10, 15+ years with MBC, managing it with lines of therapy. It is treatable, though not curable.
Part 3: Reading Your Pathology Report
After a biopsy or surgery, you get "The Report." It looks like Latin. Here is the cheat sheet:
- Histologic Grade (Nottingham Score): How "angry" do the cells look compared to normal breast cells?
- Grade 1 (Well Differentiated): Slow growing. Looks organized.
- Grade 3 (Poorly Differentiated): Fast growing. Looks chaotic.
- Ki-67 Score: The speed of cell division.
- < 20%: Low proliferation (Slow).
- > 30%: High proliferation (Fast). High Ki-67 often tips the scale toward needing chemotherapy.
- LVI (Lymphovascular Invasion): Are cancer cells seen floating in tiny blood vessels or lymph channels next to the tumor?
- Present: Higher risk of spread.
- Absent: Good sign.
- Margins:
- Negative (Clean): No ink on tumor -> The surgeon got it all.
- Positive: Cancer touches the edge -> You need a re-excision (second surgery).
Part 4: The Genomic Revolution (Oncotype DX & MammaPrint)
This is the biggest game-changer for ER+ breast cancer. In the past, everyone with a 2cm tumor got chemo "just in case." Today, we test the genes of the tumor itself.
- The Test: A sample of your tumor is sent to a lab (e.g., Genomic Health).
- The Score (0-100): It predicts the Benefit of Chemotherapy.
- Low Score (0-25): Chemo will NOT overlap hormonal therapy. You can safely skip chemo.
- High Score (> 26): Chemo is lifesaving.
- Result: This test saves thousands of women from unnecessary chemotherapy every year.
Part 5: Questions to Ask Your Oncologist
Don't go into your appointment empty-handed. Print this list.
- "What is the intent of this treatment?" (Curative vs. Palliative/Control).
- "Can I see my Oncotype or MammaPrint score?" (Crucial for Stage 1-2 ER+).
- "Am I eligible for a clinical trial?" (Trials often offeraccess to the newest 2026 drugs before they are public).
- "How will this treatment affect my fertility?" (If you are under 45).
- "Who is my nurse navigator?" (You need a point person).
Conclusion
A diagnosis is a map, not a destiny. Understanding your specific markers empowers you to ask the right questions: "Why this chemo?" "Is immunotherapy an option?" You are the captain of this ship. The storm is scary, but your compass is calibrated.



